Abstract
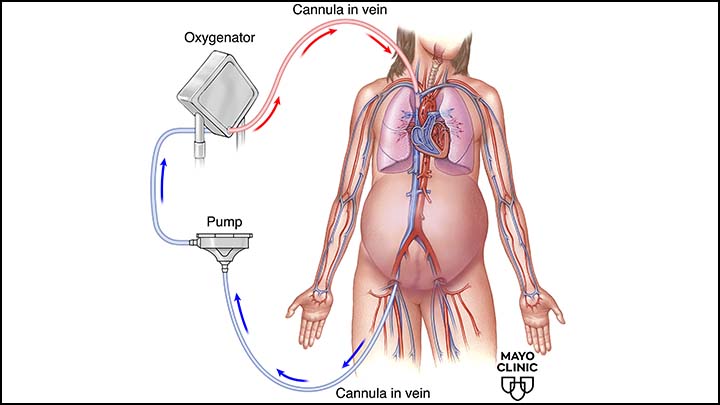
Extracorporeal membrane oxygenation (ECMO) has emerged as a life-saving intervention for critically ill pregnant patients with severe cardiopulmonary failure. Although its use in pregnancy remains rare, growing clinical experience has expanded understanding of indications, management strategies, and maternal-fetal outcomes.
Introduction
Pregnancy introduces unique physiological changes that complicate the management of severe respiratory or cardiac failure. ECMO provides temporary cardiopulmonary support, allowing time for recovery or definitive treatment. Its use in pregnancy requires balancing maternal survival with fetal well-being.
Indications for ECMO in Pregnancy
Common indications include:
- Severe acute respiratory distress syndrome
- Refractory hypoxemia
- Cardiogenic shock
- Massive pulmonary embolism
Decision-making is individualized and often time-sensitive.
Management Considerations
Key management challenges include:
- Anticoagulation balancing maternal bleeding risk
- Hemodynamic optimization for uteroplacental perfusion
- Continuous fetal monitoring when feasible
- Coordination between critical care, obstetrics, and neonatology teams
Maternal and Fetal Outcomes
Recent reports suggest improving maternal survival rates with ECMO support during pregnancy. Fetal outcomes are closely linked to gestational age at initiation and maternal stability.
Conclusion
ECMO can be a viable rescue therapy during pregnancy when conventional management fails. Multidisciplinary expertise and early intervention are crucial for optimizing outcomes for both mother and fetus.